In contrast to the heart, the lungs do not have their own pacemaker center.
2.
The lungs are inflated and deflated by the action of the rib muscles and the diaphragm. These, in turn, are activated by nerve cells located in the brain. (The muscles are striated skeletal muscles). (link)
3.
Specifically in the lower part of the brain (the medulla and the pons), there are several clusters of nerve cells that control our respiration.
4.
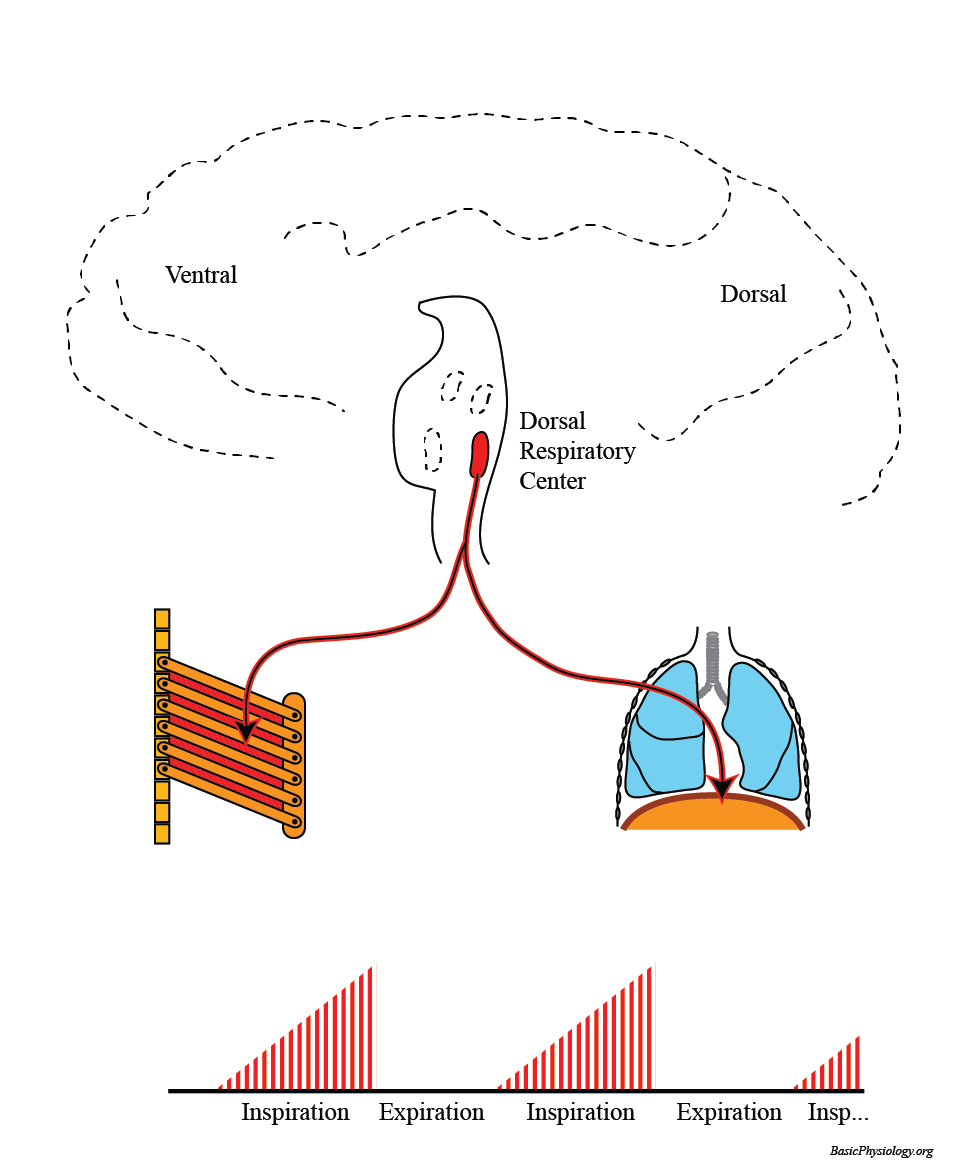
The most important cluster (or center) is the Dorsal Respiratory Center (because it is located dorsal to another center that is located more ventrally; see later).
5.
The nerve cells in the Dorsal Respiratory Center send axons to the external intercostal muscles, located between the ribs, and to the diaphragm.
6.
When these cells “fire” (make action potentials), then these action potentials will propagate to the intercostal muscles and to the diaphragm and these will then contract; this is the inspiration phase.
7.
When they stop firing, then the ribs and the diaphragm will relax and this is the (passive) expiration phase. Remember; normal expiration is passive; it does not require any action potentials and muscle contractions.
Notice the shape of the burst of action potentials in the diagram. They start very small (= very few action potentials) but the number of action potentials gradually grows until maximum is reached at the end of the inspiration. (link to smooth tetanus)
2.
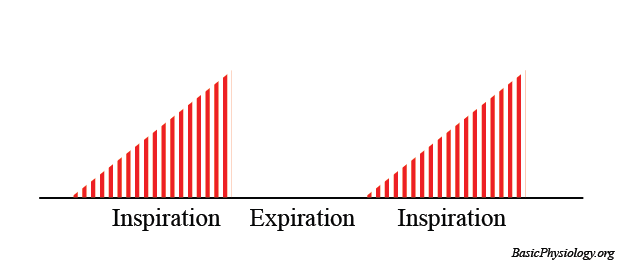
This behavior looks like a ‘ramp’; a slow and soft start followed by a progressive increase in activity until maximum is reached. This pattern has a purpose: it is good to start the inspiration slowly.
3.
Suppose that there was no ramp and that all nerve cells started to fire simultaneously, like in the right diagram.
4.
If all the neurons had started all together, then inspiration would suddenly start with a loud and strong ‘gasp’; not very nice.
5.
So, the slope of the ‘ramp’ is very important as this determines the speed and the strength of how we inspire.
Sometimes, you need to have stronger, deeper and/or a faster respiration. Then other centers will join the Dorsal Respiratory Center to control the respiration.
2.
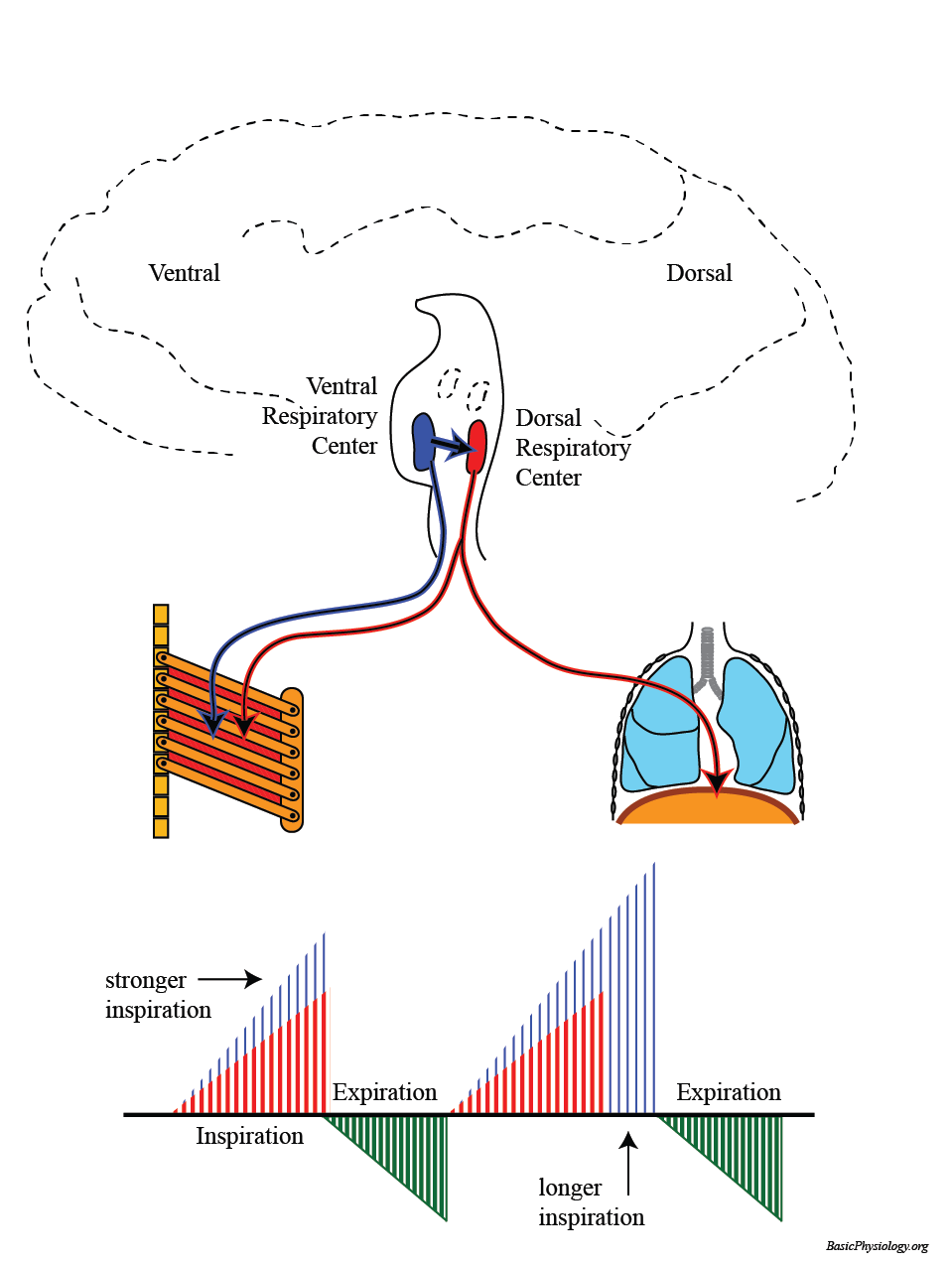
The most important additional center is the Ventral Respiratory Center. This center will join the nerve cells from the Dorsal Center in sending more action potentials.
3.
As shown in this diagram, the Ventral Respiratory Center is located close to the Dorsal Group. It sends nerve fibers to the chest but also directly to the Dorsal Group.
4.
With these additional impulses, more muscles will be excited and contract leading to a stronger inspiration.
5.
This is also indicated in the ramp signal, in blue, leading to larger amplitudes (deeper breathing) and longerduration (inspiration).
6.
Also, the expiration is now also activated because the ventral group also sends nerve fibers to muscles that will help in the expiration (green ramp).
7.
As shown in the diagram, nerves now also excite the external intercostal muscles which help the expiration.
D. Two more centers: the pneumotaxic center and the apneustic center!
Our emotions (through the hypothalamus) also affect our breathing.
2.
Emotionalhyperventilation (when you are nervous) or a sudden stop in breathing, such as when you experience an emotional shock, are good examples of these signals.
We can consciously influence our breathing (thisissomething thatyou cannot do with your heart!)
2.
These impulses therefore come from the cortex of our brain; one of the higher brain centers.
3.
But there is a (safety) limit. We can for example hold our breath (=stop breathing) for quite a long time but at a certain moment we have to gasp for fresh air! So, the lack of oxygen overrules our wish to stop breathing!
4.
Unfortunately, you can also see this in people who have drowned. They have always water in the lungs!
The chemoreceptors are sensitive to the O2, CO2 and pH concentrations in arterial blood (peripheral) and in the cerebrospinal fluid. (What is that??)
2.
In fact, the most important factor in regulating our respiration is NOT the O2 concentration but the CO2concentration!!
3.
This is because a too high CO2, produced by our body, if not swiftly expired, will influence our blood pH and thereby affect all our metabolic reactions!
4.
Therefore, an increase in CO2 must quickly be acted upon. This occurs predominantly by the central chemoreceptors (70%) but also a bit by the peripheral receptors.
5.
A too high CO2 quickly and easily crosses from the arterial blood into the cerebrospinal fluid. There, it is converted to hydrogen ions through the bicarbonate pathway.
6.
It is the hydrogen ions (pH!) that actually activate the chemoreceptor on the surface of the medulla, close to the respiratory centers.
7.
An increase in pCO2 in the blood will therefore, through this pathway, induce a strong increase in ventilation (depth and frequency). This will continue until the arterial pCO2 is back to normal (approx. 40 mmHg).
8.
As said, a less important pathway is for CO2 to activate the peripheral chemoreceptors. These are located in the wall of the aortic arch (= aortic bodies) and in the bifurcation of the carotids (=carotid bodies). (Don’t confuse them with the carotid and aortic sinus!). (link)
9.
From these peripheral chemoreceptors (or bodies), nerves go directly to the respiratory centers.
10.
Another important point about the CO2 story is the situation when the pCO2 is less than normal (less than 40 mmHg). This is important and sometimes crucial and is discussed a bit later, in “Hyperventilation”.
What is that?? Cerebrospinal fluid is the fluid inside the skulls and the vertebral column that surrounds the brain and the spinal cord.
The aortic and carotid sinuses are stretch receptors that are sensitive to the blood pressure and are discussed in the CVS chapter.
Oh yes, that is also important but not as important as CO2.
3.
For starters, there are no O2 receptors in the brain!
4.
The only O2 chemoreceptors are peripheral and located in the aortic and carotid bodies, already mentioned.
5.
Furthermore, a decrease in pO2 has only a slight effect on respiration. This is because of the shape of the oxygen saturation curve (see before). At relatively normal oxygen pressures, the curve is very flat (meaning that variations in atmospheric oxygen have little effect on saturation levels).
6.
Only when pO2 has really become very low (below 60 mmHg) will there be a strong effect on respiration.