The small intestine is actually not small at all; it is in fact the largest organ in the body and is about 5 meters long in normal adults. FIVE meters (13 feet!).
2.
It is actually much longer than the Large Intestine; which is (only) about 1.5 – 2 meters long.
3.
The reason why the two organs are called respectively ‘small’ and ‘large’ has nothing to do with their length but with their diameters; a small intestinal tube has a diameter of about 7 cm whereas the large intestine has a diameter of about 14 cm. That’s all!
4.
Back to the small intestine. As I said, this organ is actually a very long tube and consists of three parts:
the duodenum (approx. 25 cm long)
the jejunum (approx. 2 meters long)
the ileum (approx. 3 meters long).
5.
After the ileum, the digested chime (or what’s left of it) enters the cecum, the first part of the colon. This will be discussed in the next page (link).
It is at this stage important to discuss the structure of the wall of the small intestine. This wall is similar to the walls in the other GI organs and is essentially important in that it has two major functions:
motility
absorption
2.
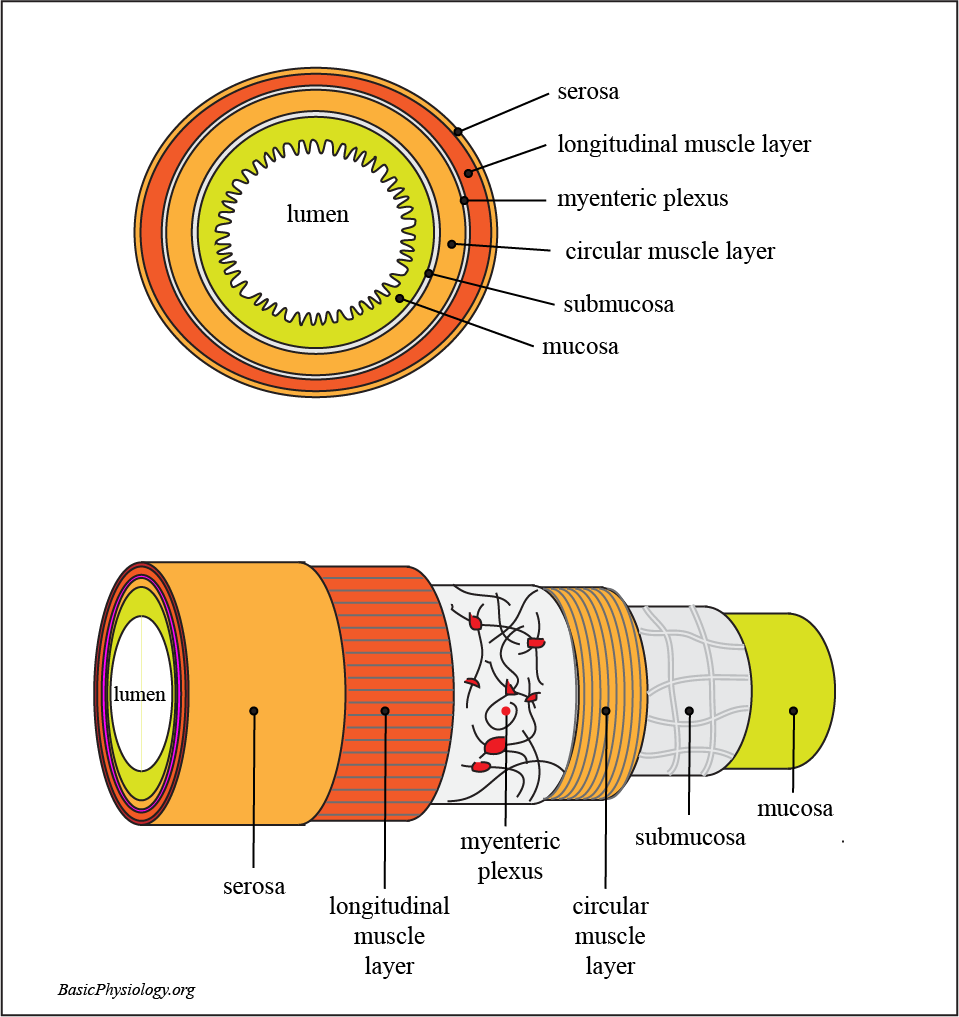
First the structure of the wall. From outside to inside:
the serosa
the longitudinal muscle layer
the myenteric plexus
the circular muscle layer
the submucosa
the mucosa
3.
The serosa is the outer layer, which protects the intestinal tube from fluids in the peritoneal cavity. It is really the ‘skin’ of the intestine.
4.
Then we have the longitudinal muscle layer. This is a relatively thin muscle layer, that runs along the length of the intestine (hence its name) and makes the intestine shorter when it contracts at a certain point.
5.
The next layer is very special; the myenteric plexus (also called Auerbach plexus). This layer contains nerve cells and other cells that control the movements, the contractions of the longitudinal and the circular muscle layers.
6.
The circular muscle layer is the thickest layer and consists of muscles that encircle the intestinal tube. When this layer contracts at a location, the tube becomes smaller.
7.
Then we have the submucosa (also called Meissner’s plexus). Just like the myenteric plexus, it contains nerve cells that control the absorption and other functions of the underlying mucosa.
8.
Finally, we have the mucosa where the most important function of the small intestine occurs; absorption of our food. To be discussed in panel E.
The intestines do not only consist of a long tube running inside the abdominal space. It also contains another structure that is of vital importance to its function; the mesentery.
2.
The mesentery is actually a very thin membrane that arises from the back of the peritoneum (= the internal lining of the abdominal cavity) and connects to the serosa of all the intestines inside the abdomen; from the cardia of the stomach all the way to the rectum.
3.
The first diagram shows the overall pattern of the mesentery, originating from the back of the abdominal cavity (vertical dashed line) and attaching itself to the borders of the organs; the major and minor curvatures of the stomach, to the small intestine (only a small part is shown here) and to the border of the large intestine; the colon. The mesentery that connects to the colon is often called mesocolon.
4.
The second diagram shows a more detailed view of the attachment of the mesentery to the wall, actually to the serosa, of an intestinal tube. This shows the reason why we have a mesentery; this is where the blood vessels, the arteries and the veins, provide the intestines with blood (I did not draw the lymphe vessels but they are also there).
5,
And, finally, also very important, the nerves that innervate the muscle layers of the intestines, necessary for producing contractions and sensory nerves to inform our brain about the local conditions in the intestines.
As in the stomach, contractions are necessary to mix the chime with the secreted juices and to ‘push’ the chime forward.
2.
In fact, this process is quite slow and it takes about 3-5 hours for the chime to travel from the pylorus to the ileo-cecal valve and into the colon.
3.
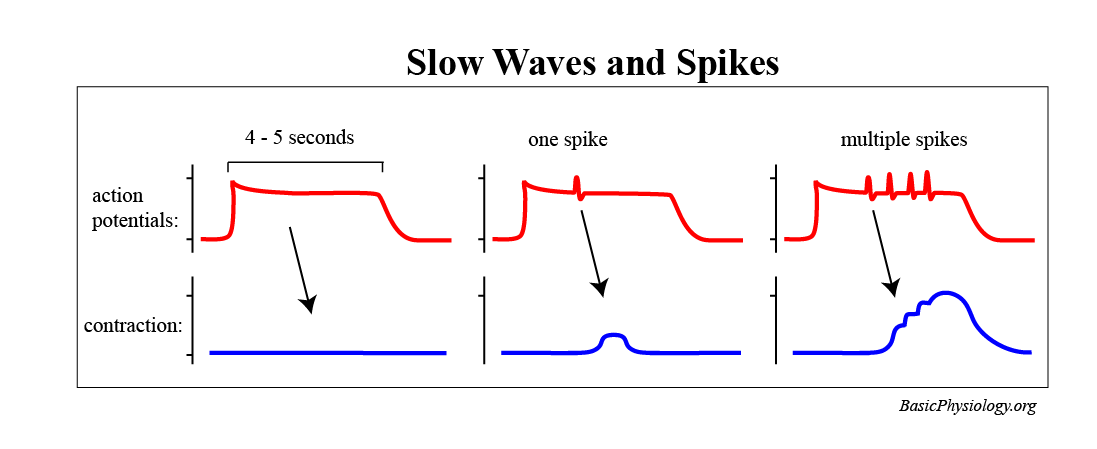
As in the heart, there is an electrical impulse propagating through the muscular wall that initiates these contractions.
4.
This is called the ‘slow wave’ (why? Because it propagates sooo slow; about 5 cm/sec; 20-50x slower than in the heart).
5.
As in the heart, this slow wave depolarizes the muscle cells but does not induce contractions. In the intestine, this depolarization, in turn, induces the occurrence of ‘spikes’.
6.
These spikes are action potentials during which calcium ions flow into the muscle cells and thereby induce contractions.
7.
It depends on the activity of the digestive nervous system how many spikes, and therefore how many and what type of contractions are induced at a particular moment.
8.
Because of these spikes, several types of contractions are possible in the small intestine (in contrast to the heart, which can only pump!).
9.
In the small intestine, these types of contractions can be roughly divided into:
As we have seen before, peristalsis is useful as it pushes the chime forward.
11. Segmentation is performed when the chime has to be mixed with the digestive juices, very much like kneading dough!
12.
Peristaltic rush is like peristalsis but propagates much faster along the intestine. This often occurs when digestion is finished and quickly pushes what’s left (usually indigestible’s) into the large intestine.
1.
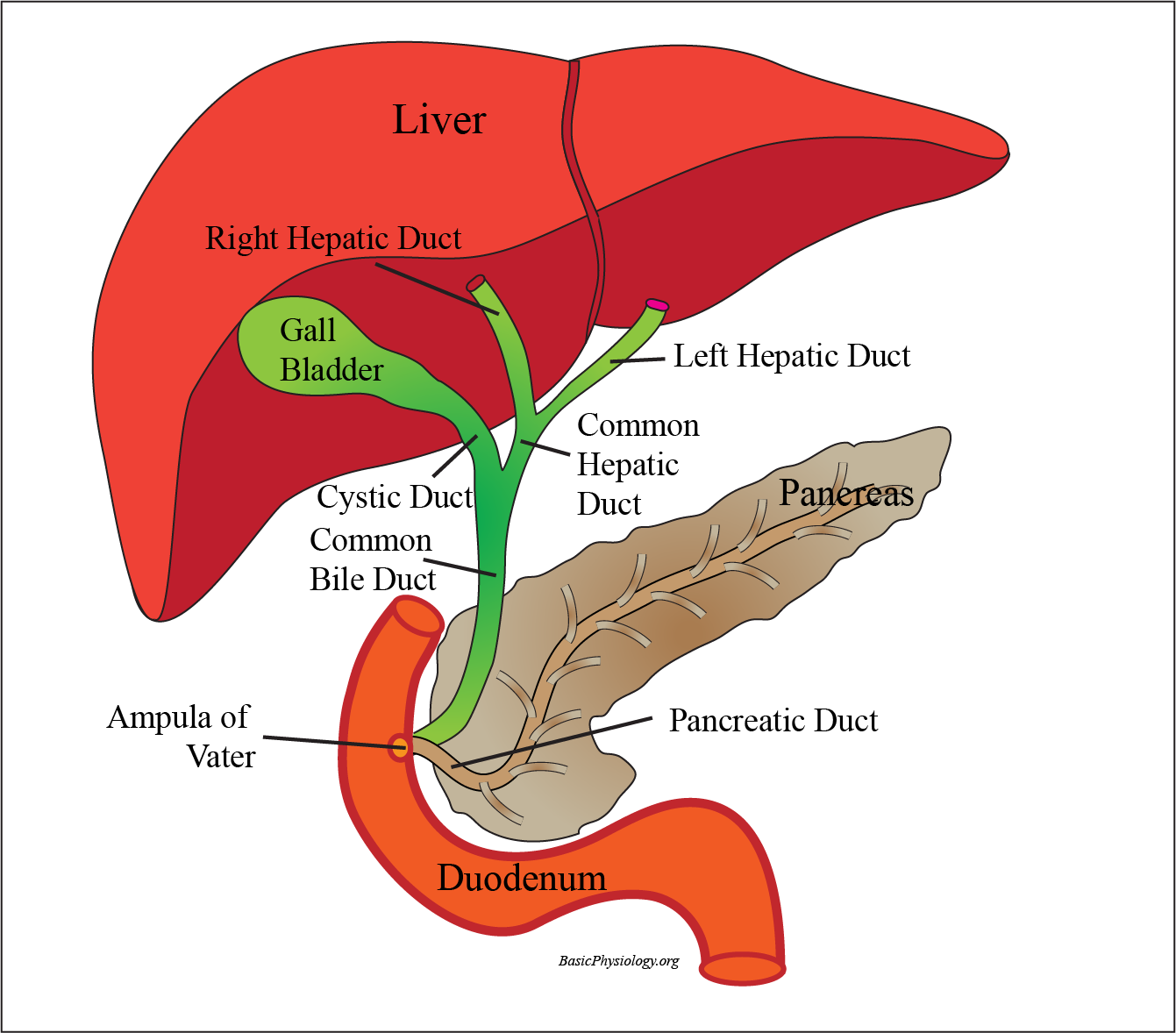
There are two other organs whose function is crucial for the digestion that is taking place in the small intestine: the liver and the pancreas.
2.
The liver is the major biochemical factory in our body (to be discussed in more details later) but here, it is important to note that the liver produces several important compounds to help digestion. These compounds together form what is called bile.
3.
This bile is secreted from both the right and the left lobe of the liver into the right and left hepatic duct.
4.
The liver produces this bile all the time, also between meals, when it is not really needed in the small intestine. In those quiet periods, the bile is accumulated in the gall bladder.
5.
But when chime arrives in the duodenum, then the gallbladder contracts and the bile is pushed into the duodenum through the common bile duct.
6.
The most important components in the bile, required for digestion, are the phospholipids. These compounds break the large lipids globules (fat) into tiny lipid fragments, smaller than one micron. This will make it easier for enzymes to digest the fat in our food.
7.
The pancreas is a very different organ, which has two functions; an endocrine organ (releasing hormones into the blood) and an exocrine function (releasing digestive enzymes into the duodenum).
8.
I am sure you all know the endocrine function of the pancreas: insulin! If you don’t have (enough) then you develop diabetes!
9.
But the exocrine secreted digestive enzymes are also very important! These enzymes digest many compounds such as proteins, starch, fat and nucleic acids.
1.
The major (no; the only) function of the small intestine is to absorb useful nutrients from our food. Without this, we would die!
2.
Remember the worm at the beginning of this chapter? (link) 80% of the worm consists of this intestine to absorb food necessary to survive.
3.
And also in humans, the small intestine is really the ‘heart’ of the GI system. The esophagus and the stomach have merely a transport, storage and some pre-digestive preparatory function while the large intestine is mainly storage before defecating!
4.
For a successful absorption, the surface area available for this absorption must be much larger than is available in a normal long small intestine.
5.
This is the task of the mucosa. Of course, there is mucosa in all the organs in the GI system but the mucosa in the small intestine is the most elaborate of all!
6.
As you can see in the diagram, the mucosa consists of circular folds (which as such already increases the surface 3x).
7.
But these folds also contain small villi, which increases the absorption area to 30x the original straight cylinder.
8.
And these villi, in turn, consist of a row of cells, microvilli, which, at their border, have multiple extensions. This further increases the absorption area to a total of 600x.
9.
So, in fact, these folds, villi and microvilli together increase the length available for absorption by 600x. If you consider the actual length of the small intestine to be 5 meters, you actually have an absorptive length of 3000 meters!!



{kind=link}
{kind=link}