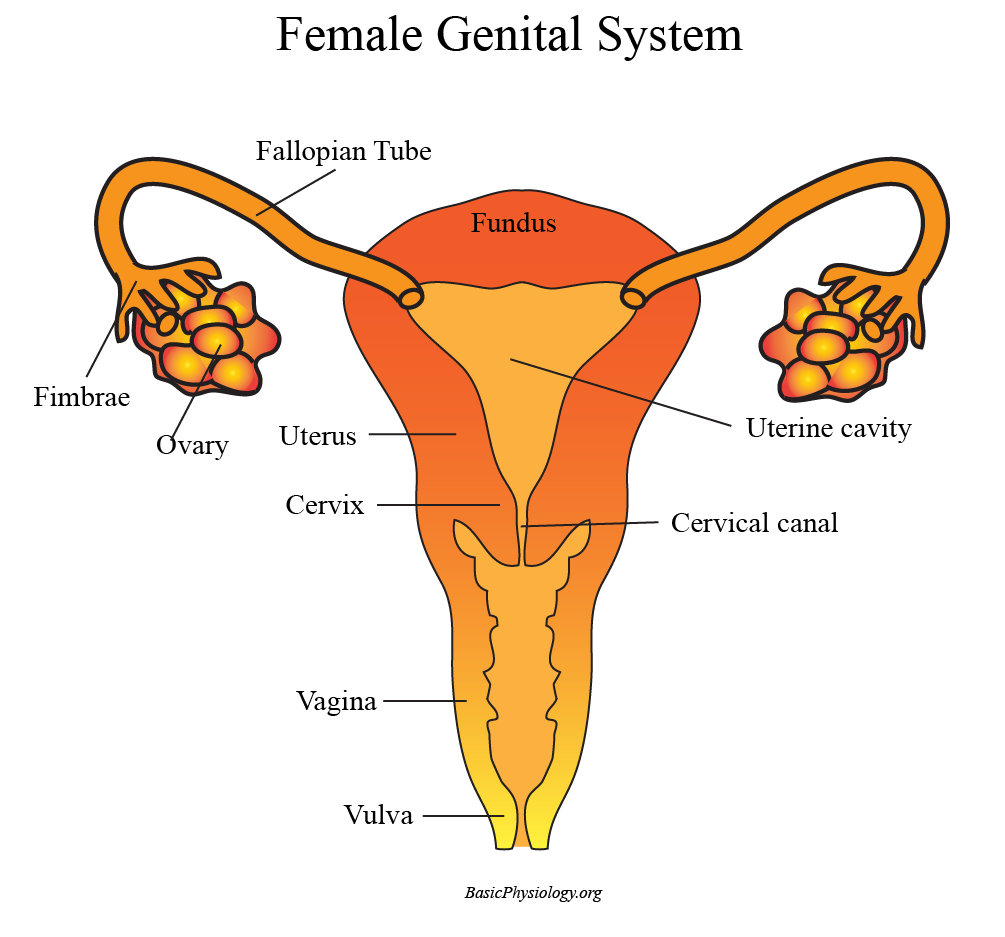
The female genital system also consists of several structures:
two ovaries
two fallopian tubes
one uterus
one cervix
one vagina
2.
The ovaries are the structures that contain the oocytes, the female ‘eggs’. In contrast to the males’ gonads however, the ovaries ‘only’ produce one or a few oocytes each month.
3.
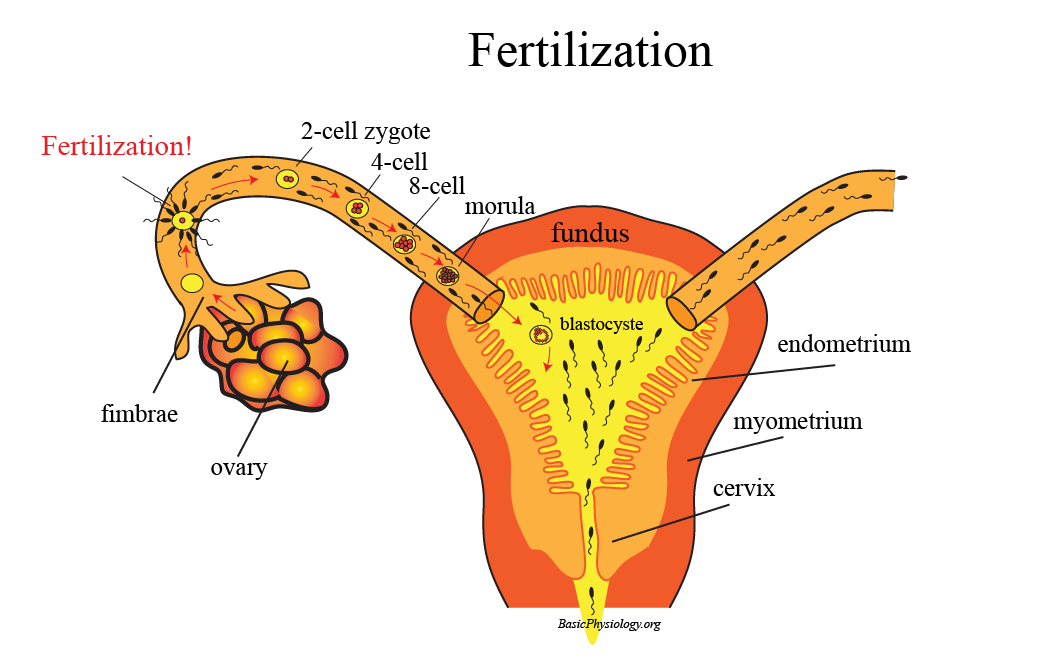
Once an oocyte is ‘mature’, it leaves the ovary and is ‘caught’ by the fimbriae and led, by peristaltic contractions, into and through the fallopian tube towards the uterine cavity.
4.
Most often, the oocyte meets a sperm cell not in the uterus but in the fallopian tube. Then the sperm cell impregnates the oocyte and an embryo formation has started.
5.
The (miniscule) embryo is further transported into the uterus where it settles against the inner wall of the uterus; the endometrium. Pregnancy has started!
We probably all now that the clitoris is the most sensitive part of the female genitalia. In fact, it is comparable to the penis gland in males.
2.
What is often unknown is that behind the clitoris and the labia’s, there is a whole genital system in women!
3.
The female internal genitalia consist of:
one clitoral gland
two corpus cavernosum
a pair of clitoris crura (=” legs”)
a pair of vestibular bulbs
4.
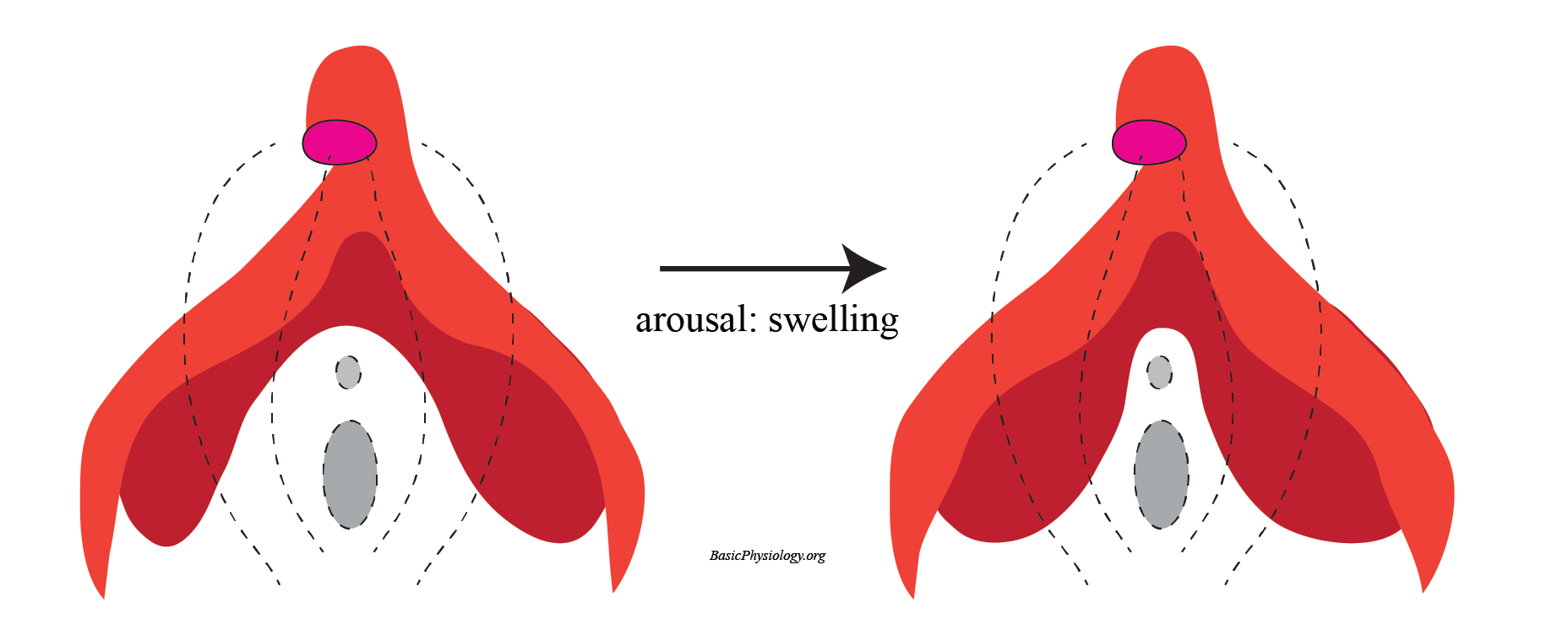
The clitoris is the external part of the clitoris gland and is highly sensitive (5-10 thousand nerve endings!). The clitoral gland lies behind the clitoris and provides for fluid upon sexual arousal.
5.
The crura of the clitoris are two “legs” running from the clitoral gland, hidden by the skin and the labial folds and surrounding the urethra and the vagina.
6.
Each crus (singular for “crura”, from the latin “leg”) is attached to a vestibular bulb and contains a corpus cavernosum.
7. Interestingly, the corpora cavernosum and the vestibular bulbs increase in size upon sexual arousal, thereby also providing pressure to the (internal) walls of the vagina which adds to the sexual pleasure.
8.
Doesn’t this “swelling” sound familiar? Yes! This is very similar to the swelling of the corpus cavernosum in the male penis!
We need to say a few words about the hymen. This, because there are so many false ideas about this rather small structure.
2.
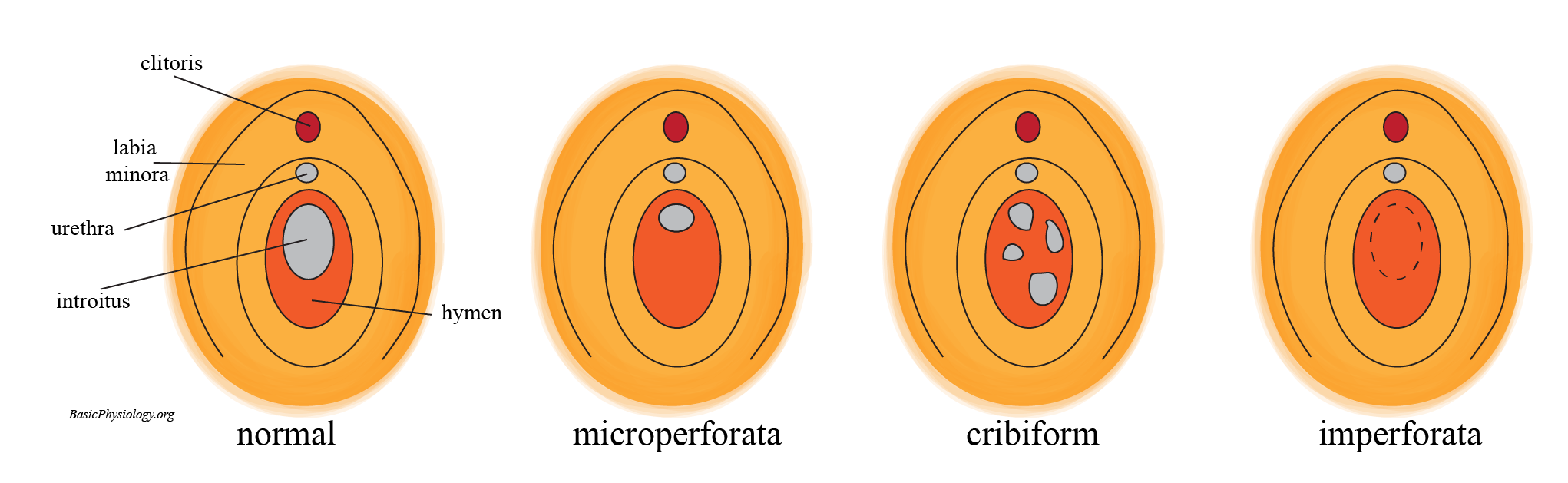
The hymen is actually a folded superficial tissue that (partially) surrounds the vaginal opening. It is also rich in nervous endings and blood vessels, which makes it sensitive to stretch and damage.
3.
The appearance of the hymen is very variable, from very small to a larger structure surrounding the whole vaginal opening.
4.
When, for the first time, coitus is performed, or an object inserted in the vagina, then the hymen is usually torn which may be painful and cause (some) bleeding.
5.
But in many women, the hymen is too small, and penetration does not cause any bleeding.
6.
Therefore, examination of a hymen cannot prove whether a female is a virgin or not.
7.
In very rare cases, the hymen covers (nearly all) of the vaginal opening (see ‘imperforata’ in the diagram), which may interfere with the monthly menstrual blood loss.
8.
In those few cases, a simple surgical incision to open up the hymen is enough to solve the problem.
9.
The hymen has little physiological significance but, unfortunately, in several societies, has acquired enormous significance.
10.
For example, it has been stated that an intact hymen proves that a woman is a virgin (which is actually very unreliable).
11.
And, in some societies, it is even possible to restore a ‘broken’ hymen by surgery.
12.
This is called hymenoplasty! This is sometimes used in some societies/religions when a woman must be a ‘virgin’ before she can marry!
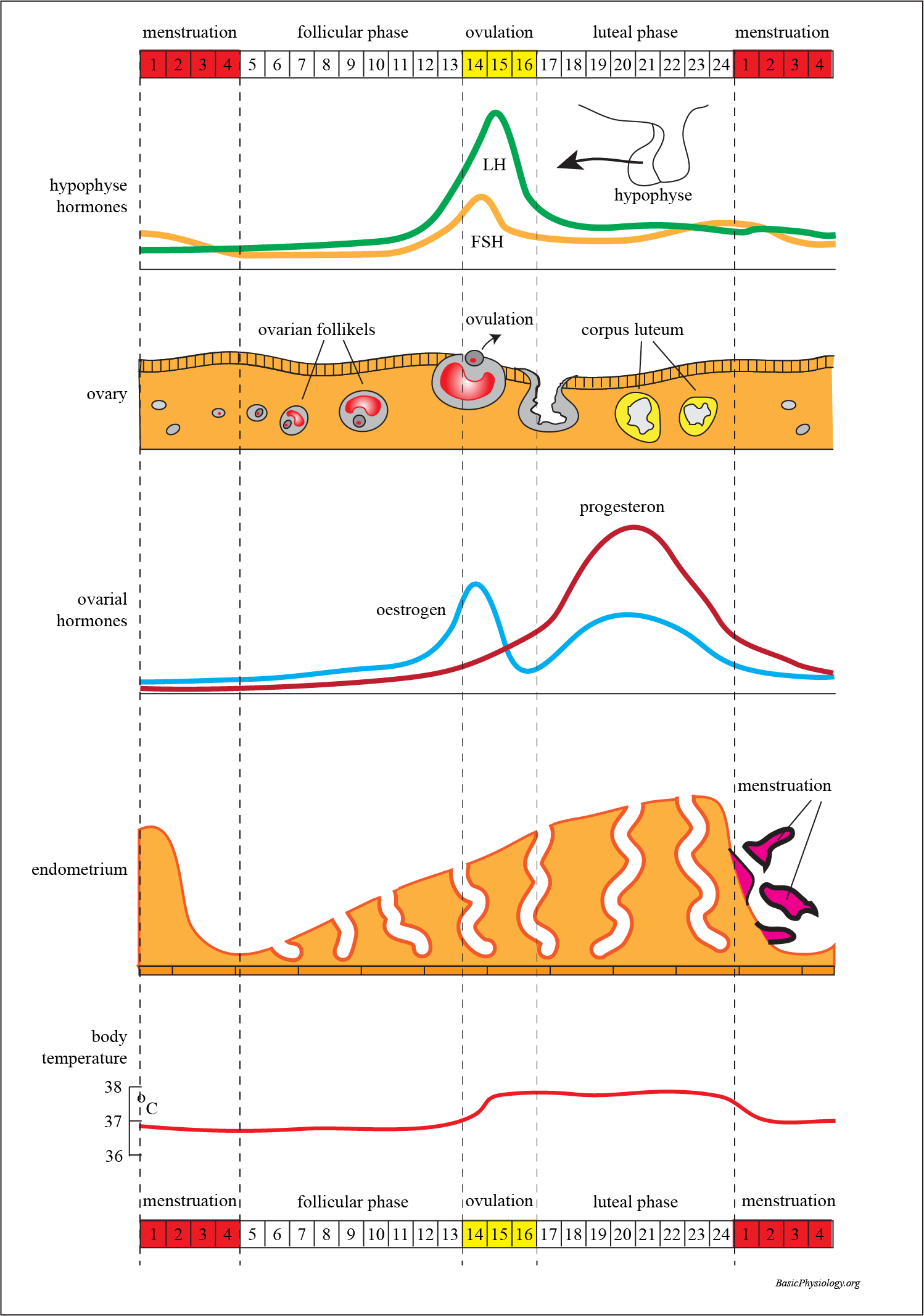
As you know, and in contrast to the male genital system, the female genital system shows a biological cycle that last approx. 24 days.
2.
During this cycle, under the influence of several hormones, the ovaries and the uterus are being stimulated to prepare for a potential pregnancy.
3.
These hormones are:
FSH (follicle stimulating hormone)
LH (luteinizing hormone)
Oestrogen
Progesterone
4.
FSH and LH are both secreted by the anterior lobe of the pituitary gland (just below the brain). In the first half of the female cycle, FSH secretion is increased (follicular phase).
5.
This increase in FSH stimulates the development of an ovarian follicle. This activated follicle will, in turn, produce oestrogen.
6.
This oestrogen, in turn, will stimulate the thickening of the endometrium in the uterus.
7.
The increase in oestrogen, in turn, will, gradually, decrease the secretion of FSH (negative feed-back).
8.
As FSH is decreasing, the secretion of LH is increasing. This will induce ovulation (the ‘liberation’ of a mature ovum), which occurs about hallway the female cycle.
9.
The structure that is left in the ovarium becomes a ‘corpus luteum’ (yellow body). This is the beginning of the second phase; the luteal phase.
10.
Now the corpus luteum secretes increasing levels of progesterone, together with increasing levels of oestrogen. These two hormones help in a further and final development of the endometrium (just in case fertilization has occurred and implantation is required).
11.
However, after several days, if nothing has happened, the LH will gradually decrease, the corpus luteum will gradually disintegrate leading to a decrease in oestrogen and progesterone.
12.
The decrease in these hormones will no longer be able to maintain the thick endometrium which will gradually disintegrate; leading to menstruation and the start of a new cycle.
Female genital mutilation involves the (partial) removal of (some) parts of the external genitalia.
2.
As you can imagine, this procedure involves lots of pain, serious bleeding, possibility of infections, and other complications.
3.
These terrible procedures are performed for non-medical reasons, such as religion, society, etc.
4.
The procedure is most often performed in young girls and creates a trauma for the rest of their lives.
5.
In many of these mutilations, the clitoris is removed by cutting it off (type 1).
6.
In other types, the minor and/or the major labia are cut away (type 2 and 3). In the ‘worst’ case, the remaining tissue is then sutured to avoid any possible insertion and leaving a small hole as an outlet for urine and menstrual blood.
7.
If the girl survives such injuries, she is also at high risk of future problems caused by the initial injury.
8.
These can be problems in urinating, or, later, in childbirth when the new baby has to pass through this area.